Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Doi:10.1016/s0140-6736(03)12950-9
Comparison of T-cell-based assay with tuberculin skin test for
diagnosis of Mycobacterium tuberculosis infection in a school tuberculosis outbreak Katie Ewer, Jonathan Deeks, Lydia Alvarez, Gerry Bryant, Sue Waller, Peter Andersen, Philip Monk, Ajit Lalvani
IntroductionIdentification and treatment of people who have latent
Background The diagnosis of latent tuberculosis infection
tuberculosis infection by targeted tuberculin skin testing
relies on the tuberculin skin test (TST), which has many
and preventive therapy is a cornerstone of tuberculosis
drawbacks. However, to find out whether new tests are better
control in developed countries.1 The main drawback of
than TST is difficult because of the lack of a gold standard test
the tuberculin skin test (TST) is poor specificity, since
for latent infection. We developed and assessed a sensitive
previous Mycobacterium bovis BCG vaccination and
enzyme-linked immunospot (ELISPOT) assay to detect T cells
environmental mycobacterial exposure can lead to false-
specific for Mycobacterium tuberculosis antigens that are
absent from Mycobacterium bovis BCG and most environmental
tuberculosis in developed countries is carried by foreign-
mycobacteria. We postulated that if the ELISPOT is a more
born immigrants from high-prevalence countries, among
accurate test of latent infection than TST, it should correlate
whom BCG vaccination and environmental mycobacterial
better with degree of exposure to M tuberculosis.
exposure are common.5,6 The TST also has severaloperational drawbacks, including the need for a return
Methods A large tuberculosis outbreak in a UK school
visit and operator-dependent variability in placement and
resulted from one infectious index case. We tested 535
reading of the test. A more accurate rapid test for latent
students for M tuberculosis infection with TST and ELISPOT.
infection is a major priority for improved tuberculosis
We compared the correlation of these tests with degree of
exposure to the index case and BCG vaccination.
The identification of genes in the M tuberculosis
genome that are absent from M bovis BCG8 and most
Findings Although agreement between the tests was high
environmental mycobacteria9 offers an opportunity to
(89% concordance, =0·72, p<0·0001), ELISPOT correlated
develop more specific tests for M tuberculosis infection.10
significantly more closely with M tuberculosis exposure than
Early secretory antigen target-6 (ESAT-6) and culture
did TST on the basis of measures of proximity (p=0·03) and
filtrate protein 10 (CFP10) are two such gene products
duration of exposure (p=0·007) to the index case. TST was
that are strong targets of the cellular immune response in
significantly more likely to be positive in BCG-vaccinated than
tuberculosis patients and contacts.11,12 The presence of
in non-vaccinated students (p=0·002), whereas ELISPOT
ESAT-6-specific T cells, detected by the rapid ex-vivo
results were not associated with BCG vaccination (p=0·44).
enzyme-linked immunospot (ELISPOT) assay forinterferon-gamma,13 is a highly sensitive and specific
Interpretation ELISPOT offers a more accurate approach
marker of M tuberculosis infection in patients who have
than TST for identification of individuals who have latent
culture-confirmed tuberculosis; its sensitivity is
tuberculosis infection and could improve tuberculosis control
substantially higher than that for the TST.14,15 In a UK
by more precise targeting of preventive treatment.
pilot study of 50 contacts at risk of latent tuberculosisinfection, we noted a correlation between ESAT-6
ELISPOT results and the extent of exposure totuberculosis cases,16 whereas unexposed people wereuniformly ELISPOT-negative.17,18
In February, 2001, a secondary school student who had
had a chronic cough for 9 months was diagnosed withsputum-smear-positive cavitatory pulmonary tuberculosis. The health authority screened 1128 of 1208 students atthe school with TST and diagnosed 69 secondary cases ofactive tuberculosis and 254 cases of latent infection. Thisoutbreak presented a unique opportunity to compare theeffectiveness of the ELISPOT assay with the TST.
In the absence of a gold standard reference test, direct
Nuffield Department of Clinical Medicine, University of Oxford, John Radcliffe Hospital, Oxford, UK (K Ewer BSc, L Alvarez PhD,
assessment of the sensitivity and specificity of a new test
A Lalvani DM); Centre for Statistics in Medicine, Institute of Health
for latent tuberculosis infection is impossible.4 However,
Sciences, Oxford, UK (J Deeks MSc); Leicestershire Health
since airborne transmission of M tuberculosis is promoted
Authority, Leicester, UK (G Bryant MFPHM, S Waller SRN,
by increasing duration and proximity of contact with an
P Monk FFPHM); and Statens Serum Institut, Copenhagen, Denmark
infectious case,19–21 a key determinant of infection is the
amount of time spent sharing room air with the source
Correspondence to: Dr A Lalvani, Nuffield Department of Clinical
case.22,23 We formed the hypothesis that if the ELISPOT
Medicine, University of Oxford, Level 7, John Radcliffe Hospital,
assay is a more sensitive and specific test than the TST, it
should correlate more closely than the TST with degree
of exposure to M tuberculosis and should be independent
THE LANCET • Vol 361 • April 5, 2003 • www.thelancet.com
For personal use. Only reproduce with permission from The Lancet Publishing Group.
of BCG vaccination status. Two measures of exposure
were prespecified at the time of study design: proximity to
the index case, based on school class and year, and hours
of direct classroom contact. Three features of this
outbreak made it particularly suitable for this
investigation: there was one infectious index case with
several hundred contacts; the outbreak occurred in an
enclosed environment; and school timetables permitted
precise quantification of the amount of time each child
Risk factors for tuberculosis exposure outside school
spent sharing room air with the source case.
The study was approved by the Leicestershire research
ethics committee. We invited 963 students, aged
11–15 years, from the same school as the index case to
participate. We obtained written informed consent from
594 (62%) children and their parents. In May and June,2001, the school nurses interviewed 550 (57% of the total
invited) of these children about place of birth and history
Heaf grade (equivalent induration after 10 TU Mantoux)
of tuberculosis exposure outside school. At the same time
they drew 10 mL blood samples that were stored in
sequentially numbered heparinised containers.
Leicestershire Health Authority screened 1128 children
with the Heaf test, in accordance with UK guidelines for
tuberculosis contacts (table 1),24 535 of whom were in our
sample of 550. Screening was done over 2 weeks, from
March 26 to April 11, 2001, 2 months after the index case
*India (44), Pakistan (nine), Bangladesh (three), Africa (Malawi, Kenya, and
Tuberculin skin testing was done by standard multiple-
Tanzania, 14), Portugal (two), and Greece, Malaysia, Sri Lanka, and Turkey (oneeach).
puncture Heaf test with a six-needle disposable-head Heaf
Table 1: Characteristics of students tested by TST and ELISPOT
gun (Bignall Surgical Instruments, Littlehampton, UK)25and concentrated purified protein derivative 100 000tuberculin units per mL (Evans Medical, Liverpool, UK),
had no access to personal identifiers or TST results.
in accordance with national guidelines.24 Heaf tests were
How ELISPOT assays are done has been previously
administered and read by the medical and nursing staff of
described;13,14 for this study we used a simplified, faster
the outbreak management team. Cutaneous induration
protocol incorporating ELISPOT plates precoated with
was scored 1 week later, in accordance with standard
monoclonal antibody to interferon-gamma (Mabtech AB,
guidelines, from grade 0 to 4.25 Generally, although the
Stockholm, Sweden), and a detector monoclonal antibody
read-out of the automated Heaf test is quantified less
to interferon-gamma preconjugated to alkaline-phosphatase
precisely than the Mantoux test—ie, grades 0–4 instead of
(Mabtech). Plates were seeded with 2·5ϫ105 peripheral
mm of induration, a continuous variable—the two tests
blood mononuclear cells per well: duplicate wells contained
generally correlate well with each other.24–26
no antigen (negative control), phytohaemagglutinin
Students who reported symptoms underwent chest
(positive control; ICN Biomedicals, OH, USA),
radiography and clinical assessment for possible active
recombinant dimeric ESAT-6 (dimESAT-6), or one of 12
tuberculosis, irrespective of skin test results.
different peptide pools derived from ESAT-6 and CFP10.
Asymptomatic students with Heaf grades 0 or 1 or Heaf
After overnight incubation at 37°C, 5% carbon dioxide ,
grade 2 and a BCG scar or documented history of BCG
plates were developed with preconjugated detector
vaccination were deemed uninfected24,25 and no action was
antibody and chromogenic substrate, BCIP/NBTPLUS (Moss
taken; students with Heaf grades 3 or 4 (irrespective of
BCG vaccination history) or grade 2 with no evidence of
Assays were scored by automated ELISPOT counter
previous BCG vaccination were deemed infected.24,25 All
(AID-GmbH, Strassberg, Germany). We scored test wells
underwent chest radiography and those with normal
as positive if they contained a mean of at least five more
radiographs were deemed to have latent tuberculosis
spot-forming cells than the mean of the negative control
infection and received 3 months’ chemoprophylaxis with
wells and this number was at least twice the mean of the
rifampicin and isoniazid. Students with abnormal
negative control wells. This cut-off14 was predefined
radiographic findings or with symptoms were further
before the results were revealed. Assays were deemed
assessed in hospital for active tuberculosis; those with
positive if there was a positive response to one or more
positive cultures for M tuberculosis from clinical samples or
pools of the ESAT-6-derived or CFP10-derived peptides,
positive radiological or clinical findings suggestive of
tuberculosis were classified as having active tuberculosis
As previously described,14 we used peptides spanning
disease. These students were treated with standard short-
the length of ESAT-6 and CFP10 (ResGen, Huntsville,
course chemotherapy for 6 months, including
AL, USA). Each peptide was 15 aminoacids long and
pyrazinamide and ethambutol for the first 8 weeks.
overlapped its adjacent peptide by 10 residues; purity was
We did ELISPOT assays in Oxford on blood samples
more than 70%. Peptides were arranged into 12 pools
from 545 of the 550 students, 2–4 h after venepuncture.
comprising two arrays of six pools each, where each array
Samples were processed and scored by two scientists who
contained all 35 peptides from both molecules in
THE LANCET • Vol 361 • April 5, 2003 • www.thelancet.com
For personal use. Only reproduce with permission from The Lancet Publishing Group.
vacated by the index case as indirectlyexposed. Direct and indirect exposure
and increase as one or both of thesemeasures increase. For latent
estimate test sensitivity and testspecificity directly, but were able to
each test to the likelihood of infection. We estimated the increase in odds
increase in exposure by logisticregression. We used matched-pairslogistic regression to assess the
Figure 1: TST and ELISPOT results for students stratified by decreasing proximity to
index case based on school year and class
T+=TST positive. T–=TST negative. E+=ELISPOT positive. ELISPOT–=ELISPOT negative.
A: students in same class as index case. B: students in classes in same year who regularly shared
lessons with index case. C: students in the four remaining classes in same year who shared only
weekly school events but no lessons with index case. D: students in different years who shared no
contrasting combinations, so that each peptide was tested
BCG vaccination, place of birth, and household
tuberculosis contact. All reported p values are two sided.
We cloned, expressed, and purified DimESAT-6 from
We investigated trends with use of the 2 statistic.
culture supernatant of recombinant Lactococcus lactis;
Comparisons between proportions were derived with
Fisher’s exact test. We did all analyses with STATA(version 7.0).
Ascertainment of exposureWe classified school students into four groups of
decreasing degrees of exposure to the index case, based on
The sponsors of the study had no role in the study
proximity and shared activities in school: the same class as
design, data collection, data analysis, data interpretation,
the index case; students in classes in the same year (year 9)
writing of the report, or in the decision to submit the
who regularly shared classes with the index case; students
in classes in the same year who shared only weekly eventswith the index case; and students in different years (7, 8,
and 10) who shared no school events with the index case
ELISPOT and TST results were available for 535
(figure 1). For students in the same school year, we used
students—44·3% of the school. Our sample was
the school timetable to quantify direct exposure to the
representative in terms of the proportion of non-white
index case, taking into account the attendance record of
children (97% in our sample vs 93% in the whole
the index case during the likely infectious period, which,
on the basis of duration of cough and associated
diagnosed with active tuberculosis (5 vs 6%); and
symptoms, was 9 months. Since the index case mixed with
participants deemed to have latent tuberculosis infection
different students for each academic subject, substantial
on the basis of TST result (24 vs 23%, table 1).
numbers of students were exposed. We classified students
The odds of a test result being positive for each
from other school years (years 7, 8, and 10) who had
increase across the four stratified exposure groups
lessons in classrooms immediately after they had been
increased by a factor of 2·78 (95% CI 2·22–3·48,
p for TST vs ELISPOT
Exposure to M tuberculosis in school Stratified exposure groups (whole school, n=535)
Direct exposure (weeks) in year 9 (n=148)
Indirect exposure (weeks) in years 7, 8, and 10 (n=387)
Risk factors for exposure to M tuberculosis outside school History of household tuberculosis contact (n=36)
*Positive result defined as Heaf grade >2 or heaf grade 2 without BCG.
Table 2: Odds ratios (95% CI) of the relations of ELISPOT and TST with intensity of M tuberculosis exposure in school and with risk factors for exposure outside school
THE LANCET • Vol 361 • April 5, 2003 • www.thelancet.com
For personal use. Only reproduce with permission from The Lancet Publishing Group.
p for vaccinated vs
*2 test for trend across all five Heaf grades.
Table 3: Effect of previous BCG vaccination on ELISPOT andTST results
p<0·0001) for the ELISPOT assay and 2·33 (1·88–2·88,
p<0·0001) for the TST. The ELISPOT assay correlated
Figure 2: Stratification of TST-positive students with
significantly better with increasing exposure across the
presumed latent tuberculosis infection by ELISPOT result
four groups than did the TST (p=0·03; figure 1, table 2).
128 TST-positive students with no clinical or radiographical signs of
Direct exposure of the 148 children in year 9 ranged
active tuberculosis disease. Each circle represents one student:white=students with direct classroom exposure to index case;
from 0 to 17 school weeks: 57 students had some direct
classroom exposure, with a median of 2·2 school weeks(IQR 1·4–13·4). The odds of a positive ELISPOT result
(p=0·002), with substantially more Heaf grade 3 (81 of
increased by a factor of 2·51 (1·58–3·99, p<0·0001) with
467 vs 2 of 68, p=0·001), and grade 2 results in BCG-
each week of direct exposure, which was significantly
higher (p=0·007) than that for the TST (odds ratio 1·30
Of the 128 participants presumed to have latent
[95% CI 1·10–1·54], p=0·002; table 2).
tuberculosis infection on the basis of a positive TST
Of the 387 children in years 7, 8, and 10, 196 pupils
with no evidence of active tuberculosis, 97 (76%)
had indirect exposure, up to a maximum of 1·16 weeks.
tested positive with ELISPOT. This ELISPOT-positive
Although ELISPOT and TST were more likely to be
subgroup had significantly higher Heaf grades and
positive with increasing exposure, neither showed a
significantly more exposure to M tuberculosis than did the
ELISPOT-negative students. Heaf grades were
ELISPOT assay and TST were positively correlated
significantly higher among ELISPOT-positive students
with a history of household tuberculosis contact (n=36,
than among ELISPOT-negative students (p<0·0001,
table 2). 76 children were born in countries with a high
figure 2). In the ELISPOT-positive group there were
prevalence of tuberculosis and climates associated with
significantly more students with direct exposure to the
increased exposure to environmental mycobacteria (table
index case than in the ELISPOT-negative group (35 of
1). The mean duration of residence in these countries
97 vs one of 31, p<0·0001; figure 2).
was 7·8 years. TST results, but not ELISPOT results,
Agreement between TST and ELISPOT was high
were significantly associated with birth in one of these
(=0·72 [95% CI 0·64–0·80], p<0·0001), with
concordant results in 475 (89%) students (table 4). For
For 362 students, the date of BCG vaccination was
students in whom test results were discordant, it is
documented in the Leicestershire Health Authority
impossible to know for certain which test was correct
records, of whom 323 were vaccinated at birth. An
because there is no reference test. However, table 4
additional 105 students had BCG scars but the date of
shows that an isolated positive ELISPOT result (ie, one
vaccination was not available because they were born
associated with a negative TST) was a strong predictor of
outside Leicester; 101 were born in countries where BCG
M tuberculosis exposure, whereas an isolated positive TST
vaccination is given at birth. Therefore 424 (91%) of 467
result was not. This finding suggests that isolated positive
BCG-vaccinated students were vaccinated at birth. The
ELISPOT results are more likely to be true positives than
ELISPOT assay showed no significant relation with BCG
are isolated positive TST results. For students with
vaccination status (p=0·44, table 3). By contrast, BCG-
positive TST and ELISPOT results, the relative risk of
vaccinated children were significantly more likely to have
direct exposure to the index case, compared with that for
higher Heaf grades than unvaccinated children
students with negative TST and ELISPOT, was 17·6
Students’ exposure to M tuberculosis
pTST–/ELISPOT+ vs TST– ELISPOT–*
TST+/ELISPOT– vs TST– ELISPOT–*
NT=no statistical test undertaken due to skewed distributional shape because most students had no direct exposure. *p values are for comparison of epidemiologicalcharacteristics of students with an isolated positive test result vs characteristics of students negative for both tests.
Table 4: Analysis of concordant and discordant test results
THE LANCET • Vol 361 • April 5, 2003 • www.thelancet.com
For personal use. Only reproduce with permission from The Lancet Publishing Group.
The high specificity of ELISPOT might explain the
strong relation between positive ELISPOT results andTST induration size in individuals who have positive TSTresults. The size of the TST response is positivelyassociated with higher tuberculosis case rates duringfollow-up; thus, the ELISPOT assay may have identifiedthe subgroup of TST-positive individuals who actuallyhave latent tuberculosis infection. These individuals aredistinct from those whose weakly positive TST responsesrepresent false-positive results due to antigenic crossreactivity of purified protein derivative. Moreover, theELISPOT-positive group had substantially more exposureto M tuberculosis than did the ELISPOT-negative group. This improved specificity of the ELISPOT could help toavoid unnecessary chemoprophylaxis in uninfectedindividuals; this ability to screen out false-positive TSTresults will become increasingly important as theprevalence of latent infection falls in low-prevalence
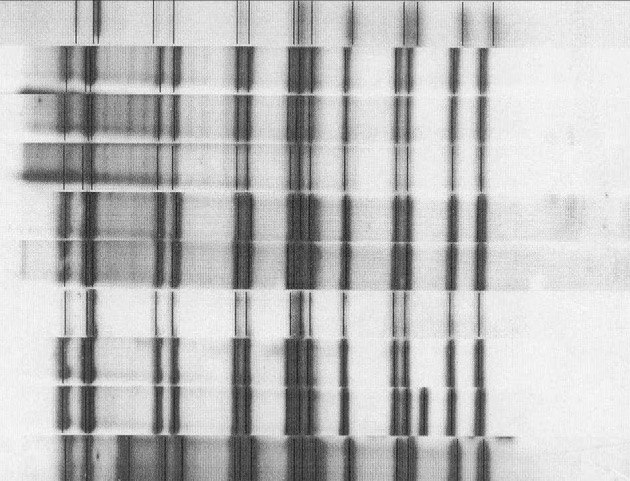
Figure 3: Restriction fragment length polymorphism patterns of
M tuberculosis isolates from students at school
derivative may explain why a new whole-blood interferon-
Top row is isolate from index case; other nine rows are isolates from
gamma ELISA based on purified protein derivative
secondary cases from who M tuberculosis was cultured.
There is compelling evidence that the outbreak we
(95% CI 8·1–38·0, p<0·001); for those with negative
studied was due to one index case, who was the first
TST and positive ELISPOT results it was 11·7
symptomatic case of pulmonary tuberculosis in the
(4·2–33·2, p<0·001); and for those with postive TST and
school.30 The molecular epidemiology also suggests that
negative ELISPOT results, it was 2·97 (0·6–13·7,
this was a point-source outbreak. Only two other children
Molecular strain typing by variable-number tandem
symptomatic for less than 2 weeks before admission to
repeat, mycobacterial interspersed repetitive unit, and
hospital and both were in year 11, which did not
spoligotyping showed that all nine secondary isolates of
participate in the study. Moreover, their M tuberculosisM tuberculosis from students at the school were identical
isolates were identical to that of the index case by all four
to that of the index case. IS6110-based restriction
fragment length polymorphism (figure 3) showed that
The high rates of tuberculosis infection and disease at
seven of the nine secondary isolates were identical to that
the school are unlikely to merely reflect the epidemiology
of the index case, whereas two were very similiar,
of tuberculosis in the local community. First, this outbreak
differing by one and three bands each.
accounted for a third of all tuberculosis cases in Leicesterin 2001. Second, all 1226 household contacts of the
69 tuberculosis cases and 254 cases of latent tuberculosis
In the absence of a gold standard test for latent
infection were screened by the health authority and no
tuberculosis infection, the sensitivity and specificity of the
cases of infectious pulmonary tuberculosis were identified.
ELISPOT assay or the TST cannot be directly
Third, four other Leicester schools were screened by TST,
quantified.4 However, given that the likelihood of latent
and the rates of positive skin tests were 1–4%. Fourth,
tuberculosis infection is determined by exposure to
when year 8 students at this school underwent Heaf testing
M tuberculosis,19–23 we were able to rank the tests according
to their diagnostic accuracy. Agreement between TST and
The minimum exposure to an infectious person that is
ELISPOT results was high, but discordance in 11% of
required for M tuberculosis transmission is unknown, but
students shows that the tests are not equivalent. Our
must be low, since many well-documented cases of
results indicate that ELISPOT probably has higher
infection result from brief exposure31 and many students
sensitivity and specificity than TST. First, the significantly
who did not share lessons with the source case must have
closer correlation of ELISPOT than TST with degree of
acquired infection in this way. The amount of exposure
exposure to M tuberculsosis suggests a higher sensitivity for
required before transmission of M tuberculosis becomes
detection of latent infection. Second, TST, but not
inevitable is also unknown. Since all students with 5 or
ELISPOT, was confounded by BCG vaccination, despite
more school-weeks of exposure had positive results on the
11–15 years having elapsed since vaccination, which
ELISPOT assay, however, our findings suggest that 130 h
suggests a higher specificity for the ELISPOT assay.
sharing room air with a person with sputum smear-
TST and ELISPOT were more likely to be positive in
positive cavitatory tuberculosis is certain to result in
students who had a history of household tuberculosis
contact, a marker of M tuberculosis exposure outside
Longitudinal assessment of the positive predictive
school, than in students without such a history. By
value of this assay for subsequent development of active
contrast, for the students born in high-prevalence
tuberculosis will be necessary. In one report workers
countries, mainly Africa and Asia (a risk factor for
suggest that T-cell responses to ESAT-6 in healthy
environmental myobacterial exposure3,4 and M tuberculosis
contacts are associated with subsequent active disease.32
exposure) only the TST was significantly more likely to be
Students in our study who had positive ELISPOT but
positive. Given that the ELISPOT assay correlates
negative TST results, who have not had chemoprophylaxis,
strongly with all other measures of M tuberculosis
are receiving close clinical and radiographic follow-up.
exposure, its independence from foreign birth suggests
We used the Heaf test, because it is used for tuberculin
that, unlike TST, it is not confounded by environmental
testing in contact investigations in the UK, and is
stipulated in national guidelines.24 Since the Mantoux
THE LANCET • Vol 361 • April 5, 2003 • www.thelancet.com
For personal use. Only reproduce with permission from The Lancet Publishing Group.
method is more widely used internationally, ELISPOT
Taylor Z, O’Brien RJ. Tuberculosis elimination: are we willing to pay
should be compared in the future with this method; we
the price? Am J Respir Crit Care Med 2001; 163: 1–2.
have recently started such studies in several countries.
Mahairas GG, Sabo PJ, Hickey MJ, Singh DC, Stover CK. Molecular
ELISPOT gives quantitative results the morning after
analysis of genetic differences between Mycobacterium bovis BCG and virulent M bovis. J Bacteriol 1996; 178: 1274–82.
taking a blood sample and is more convenient, objective,
Harboe M, Oettinger T, Wiker HG, Rosenkrands I, Andersen P.
and rapid than the TST. Although TST is cheap, related
Evidence for occurrence of the ESAT-6 protein in Mycobacterium
indirect costs are associated with return visits and the
tuberculosis and virulent Mycobacterium bovis and for its absence in
trained staff required to administer and read the test. Mycobacterium bovis BCG. Infect Immun 1996; 64: 16–22.
10 Andersen P, Munk ME, Pollock JM, Doherty TM. Specific immune-
Introduction of ELISPOT might initially increase the cost
based diagnosis of tuberculosis. Lancet 2000; 356: 1099–104.
of tuberculosis control, but the savings that would follow
11 Lein AD, von Reyn CF, Ravn P, Horsburgh CR Jr, Alexander LN,
from improved diagnosis of latent tuberculosis infection
Andersen P. Cellular immune responses to ESAT-6 discriminate
could make it very cost effective in the long term. Better
between patients with pulmonary disease due to Mycobacterium avium
detection of latent infection would lessen the number of
complex and those with pulmonary disease due to Mycobacterium tuberculosis. Clin Diagn Lab Immunol 1999; 6: 606–09.
cases of active tuberculosis and, therefore, the attendant
12 Arend SM, Andersen P, van Meijgaarden KE, et al. Detection of
cost of diagnosis, hospital admission and contact tracing.
active tuberculosis infection by T cell responses to early-secreted
Fewer false-positive results in uninfected contacts
antigenic target 6-kDa protein and culture filtrate protein 10.
would avoid the costs associated with unnecessary
J Infect Dis 2000; 181: 1850–54.
chemoprophylaxis and its associated toxic effects.
13 Lalvani A, Brookes R, Hambleton S, Britton WJ, Hill AV,
McMichael AJ. Rapid effector function in CD8+ memory T cells. J Exp Med 1997; 186: 859–65.
14 Lalvani A, Pathan AA, McShane H, et al. Rapid detection of
Ajit Lalvani, Katie Ewer, Jonathan Deeks, Gerry Bryant, and Philip Monk
Mycobacterium tuberculosis infection by enumeration of antigen-
designed the study. Ajit Lalvani coordinated the study. Katie Ewer and
specific T cells. Am J Respir Crit Care Med 2001; 163: 824–28.
Lydia Alvarez did the ELISPOT assays. Sue Waller interviewed and enrolled
15 Barnes PF. Diagnosing latent tuberculosis infection: the 100-year
all the participants. Demographic information was obtained and recorded by
upgrade. Am J Respir Crit Care Med 2001; 163: 807–8.
Sue Waller, Gerry Bryant, and Philip Monk. Jonathan Deeks computed the
16 Lalvani A, Pathan AA, Durkan H, et al. Enhanced contact
duration of exposure and did the statistical analysis. Peter Andersen
tracing and spatial tracking of Mycobacterium tuberculosis infection
synthesised the recombinant ESAT-6 and provided technical advice and
by enumeration of antigen-specific T cells. Lancet 2001; 357:
support. Ajit Lalvani wrote the paper with help from Katie Ewer and
Jonathan Deeks, and all researchers reviewed the final report.
17 Lalvani A, Nagvenkar P, Udwadia Z, et al. Enumeration of T cells
specific for RD1-encoded antigens suggests a high prevalence of
latent Mycobacterium tuberculosis infection in healthy urban Indians.
AL is the named inventor on several patents related to T-cell-based
J Infect Dis 2001; 183: 469–77.
diagnosis filed by the University of Oxford since 1996. Regulatory
18 Chapman AL, Munkanta M, Wilkinson KA, et al. Rapid detection of
approval and commercialisation of the ELISPOT assay will be undertaken
active and latent tuberculosis infection in HIV-positive individuals by
by a spin-out company of the University of Oxford (Oxford Immunotec),
enumeration of Mycobacterium tuberculosis-specific T cells. AIDS
in which AL has an equity stake. PA is the named inventor of several
2002; 16: 2285–93.
patents filed by Statens Serum Institute relating to the discovery of M
19 Grzybowski S, Barnett GD, Styblo K. Contacts of cases of active
tuberculosis-specific antigens.
pulmonary tuberculosis. Bull Int Union Tuberc 1975; 50: 90–106.
20 Stead WW. Undetected tuberculosis in prison. Source of infection for
community at large. JAMA 1978; 240: 2544–47.
We thank the students for their participation; Gary Coleby, Alan Anderson,
21 Kenyon TA, Valway SE, Ihle WW, Onorato IM, Castro KG.
Isobel Pearce, Dean Barnett and the staff of Crown Hills Community
Transmission of multidrug-resistant Mycobacterium tuberculosis during
College for their generous cooperation; Lorna Briars, Elaine Weare,
a long airplane flight. N Engl J Med 1996; 334: 933–38.
Alison Woodbridge, and Fiona Booth for interviewing and drawing blood
22 Houk VN, Baker JH, Sorensen K, Kent DC. The epidemiology of
samples from the students; Debbie Modha, Judith West, Wren Hoskyns,
tuberculosis infection in a closed environment. Arch Environ Health
Louise Coole, Helen Thuraisingham, Ginder Narle, Niru Rana,
1968; 16: 26–35.
Lindsey Abbott, Vicki Lowe, and Barbara Smithson for epidemiological
23 Houk VH, Kent DC, Baker JH, Sorensen K, Hanzel GD. The Byrd
information from the outbreak investigation; Francis Drobniewski and
study: in-depth analysis of a micro-outbreak of tuberculosis in a
Malcolm Yates of the Mycobacterial Reference Library, London, for RFLP
closed environment. Arch Environ Health 1968; 16: 4–6.
typing; John Watson of the Communicable Disease Surveillance Centre for
24 Joint Tuberculosis Committee of the British Thoracic Society.
facilitating the project and valuable advice; Doug Altman, Constantine
Control and prevention of tuberculosis in the United Kingdom: code
Gatsonis, Patrick Bossuyt, and Les Irwig for guidance in planning the
of practice 2000. Thorax 2000; 55: 887–901.
statistical analysis; Peter Barnes, Luca Richeldi, Peter Wrighton-Smith,
25 Department of Health. Immunisation against infectious disease.
Shabbar Jaffar, Paul Newton, Liz Corbett, and Anthony Butterworth for
London: H M Stationery Office, 1996.
helpful discussions; Ramilla Mistry and Dina Shah for translations; and
26 Carruthers KJ. Comparison of the Heaf (multiple puncture)
Ansar Pathan, Katalin Wilkinson and Tilly Pillay for laboratory assistance.
and Mantoux tests using several tuberculins. Tubercle 1969; 50:
This study was funded by the Wellcome Trust. AL is a Wellcome senior
research fellow in clinical science.
27 Deeks JJ. Systematic reviews of evaluations of diagnostic and
screening tests. In: Egger M, Davey-Smith G, Altman D, eds.
Systematic reviews in health care: meta-analysis in context. London:
Targeted tuberculin testing and treatment of latent tuberculosis
infection: joint statement of the American Thoracic Society (ATS) and
28 Brock I, Munk ME, Kok-Jensen A, Andersen P. Performance of
the Centers for Disease Control and Prevention (CDC).
whole blood IFN-gamma test for tuberculosis diagnosis based on
Am J Respir Crit Care Med 2000; 161: S221–47.
PPD or the specific antigens ESAT-6 and CFP-10. Int J Tuberc Lung
Huebner RE, Schein MF, Bass JB, Jr. The tuberculin skin test.
Dis 2001; 5: 462–67. Clin Infect Dis 1993; 17: 968–75.
29 Mazurek GH, LoBue PA, Daley CL, et al. Comparison of a whole-
Black GF, Weir RE, Floyd S, et al. BCG-induced increase in
blood interferon gamma assay with tuberculin skin testing for
interferon-gamma response to mycobacterial antigens and efficacy of
detecting latent Mycobacterium tuberculosis infection. JAMA 2001;
BCG vaccination in Malawi and the UK: two randomised controlled
286: 1740–47.
studies. Lancet 2002; 359: 1393–401.
30 Press releases. http://www.leics-ha.org.uk (accessed March 18, 2003).
Jasmer RM, Nahid P, Hopewell PC. Clinical practice: latent
31 Small PM, Hopewell PC, Singh SP, et al. The epidemiology of
tuberculosis infection. N Engl J Med 2002; 347: 1860–66.
tuberculosis in San Francisco: a population-based study using
Zuber PL, McKenna MT, Binkin NJ, Onorato IM, Castro KG.
conventional and molecular methods. N Engl J Med 1994; 330:
Long-term risk of tuberculosis among foreign-born persons in the
United States. JAMA 1997; 278: 304–07.
32 Doherty TM, Demissie A, Olobo J, et al. Immune responses to the
Rose AM, Watson JM, Graham C, et al. Tuberculosis at the end of
Mycobacterium tuberculosis-specific antigen ESAT-6 signal subclinical
the 20th century in England and Wales: results of a national survey in
infection among contacts of tuberculosis patients. J Clin Microbiol
1998. Thorax 2001; 56: 173–79.
2002; 40: 704–60.
THE LANCET • Vol 361 • April 5, 2003 • www.thelancet.com
For personal use. Only reproduce with permission from The Lancet Publishing Group.
La maladie de Crohn Introduction La maladie de Crohn (MC) est la principale maladie inflammatoire chronique de l'intestin de cause à ce jour inconnue. El e est, en France, un problème de santé publique parce que : a) c'est une maladie fréquente dont la prévalence chez l'adulte et l'incidence chez l'enfant augmentent; b) el e at eint des sujets jeunes (pic d'incidence entre 18 et
MIGRAÑAS ¿Qué son las migrañas? Las migrañas, también llamadas jaquecas, son fuertes dolores de cabeza que pueden llegar a ser muy incapacitantes. El dolor suele durar varias horas e incluso días. Generalmente el dolor es pulsátil, como el bombeo del corazón, ocurre habitualmente en un lado de la cabeza, aunque puede generalizarse, y típicamente empeora con los movimien
 The high specificity of ELISPOT might explain the
strong relation between positive ELISPOT results andTST induration size in individuals who have positive TSTresults. The size of the TST response is positivelyassociated with higher tuberculosis case rates duringfollow-up; thus, the ELISPOT assay may have identifiedthe subgroup of TST-positive individuals who actuallyhave latent tuberculosis infection. These individuals aredistinct from those whose weakly positive TST responsesrepresent false-positive results due to antigenic crossreactivity of purified protein derivative. Moreover, theELISPOT-positive group had substantially more exposureto M tuberculosis than did the ELISPOT-negative group.
The high specificity of ELISPOT might explain the
strong relation between positive ELISPOT results andTST induration size in individuals who have positive TSTresults. The size of the TST response is positivelyassociated with higher tuberculosis case rates duringfollow-up; thus, the ELISPOT assay may have identifiedthe subgroup of TST-positive individuals who actuallyhave latent tuberculosis infection. These individuals aredistinct from those whose weakly positive TST responsesrepresent false-positive results due to antigenic crossreactivity of purified protein derivative. Moreover, theELISPOT-positive group had substantially more exposureto M tuberculosis than did the ELISPOT-negative group.