Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Nntonline.com
REGULAR SALMETEROL IN CHRONIC ASTHMA: SERIOUS
An editorial by Kevin Weiss in the Annals of Internal Medicine(1) has warned against the use of long-acting beta2-agonists (with or without inhaled corticosteroids) as first line treatment in asthma, and especially not for people with mild asthma. He also suggests that it would be prudent to use long-acting beta2-agonists only when the prescriber is confident that the user will adhere to close monitoring and instructions to seek further care when asthma is out of
This conclusion comes in response to a meta-analysis of GlaxoSmithKline trials in which regular salmeterol was given to people with asthma in combination with inhaled corticosteroids (2).
We have published a Cochrane review(3) looking at all the trials in which salmeterol was compared to placebo or regular short-acting beta2-agonists, but where inhaled corticosteroids were not part of the randomised treatment. The findings of the review are explained in a he full text of the review is also available
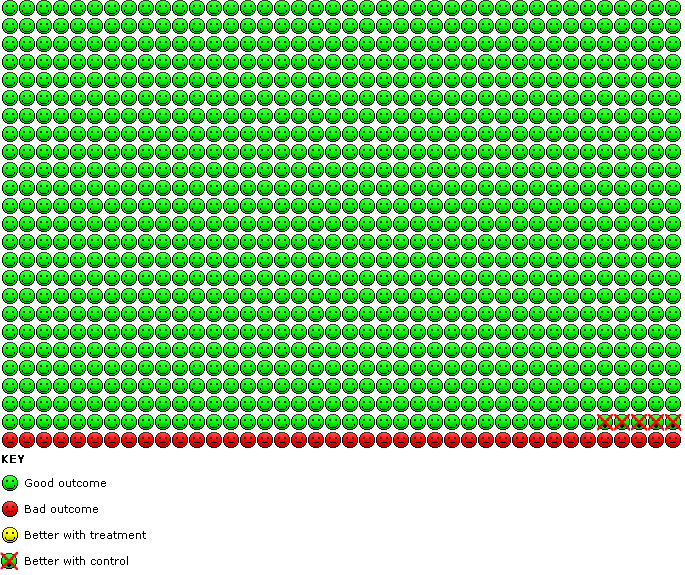
There was a significant increase in serious adverse events of any cause when regular salmeterol was compared to placebo; whereas the placebo group suffered around 40 events for every 1000 patients treated, this rose to 45 events with regular salmeterol (over a four to six month
By combining the data on asthma deaths from the two very large surveillance studies (4, 5) we found that those who were not taking inhaled corticosteroids when they were enrolled into the trial suffered around 12 extra asthma deaths with regular salmeterol, compared to around 2
extra asthma deaths in those who were taking inhaled corticosteroids. However, this does not prove that inhaled corticosteroids abolish the risk with regular salmeterol, as the confidence interval included the possibility of a three-fold increase in asthma deaths even with inhaled corticosteroids were used.
In a nutshell the conclusions that we came to are very similar to those of Kevin Weiss. The risks as well as the benefits of salmeterol should be considered when deciding whether long-acting beta2-agonists are to be used in chronic asthma.
Weiss KB. Drug safety and salmeterol: the controversy continues. Ann Intern Med2008
Bateman E, Nelson H, Bousquet J, Kral K, Sutton L, Ortega H, et al. Meta-analysis: Effects
of Adding Salmeterol to Inhaled Corticosteroids on Serious Asthma-Related Events. Ann Intern
Cates CJ, Cates MJ. Regular treatment with salmeterol for chronic asthma: serious
adverse events (Cochrane Review). Cochrane Database of Systematic Reviews2008(3).
Castle W, Fuller R, Hall J, Palmer J. Serevent nationwide surveillance study: comparison
of salmeterol with salbutamol in asthmatic patients who require regular bronchodilator
treatment. BMJ (Clinical research ed1993;306(6884):1034-7. 5.
Nelson HS, Weiss ST, Bleecker ER, Yancey SW, Dorinsky PM, the SMART Study Group.
The Salmeterol Multicenter Asthma Research Trial: A Comparison of Usual Pharmacotherapy for Asthma or Usual Pharmacotherapy Plus Salmeterol. Chest2006 January 1, 2006;129(1):15-
Publications (2008-2009) 1. Kraiczy, P ., Seling, A., Brissette, C. A., Rossmann, E., Hunfeld, K.-P., Bykowski, T., Burns, L. H., Troese, M. J., Cooley, A.E., Miller, J. C., Brade, V., Wallich, R., Casjens, S., and B. Stevenson. Antibodies against Borrelia burgdorferi complement regulator-acquiring surface protein 2 (CspZ) as a serological marker of human Lyme disease. Clin. Vaccine Immun
 Weiss KB. Drug safety and salmeterol: the controversy continues. Ann Intern Med2008
Bateman E, Nelson H, Bousquet J, Kral K, Sutton L, Ortega H, et al. Meta-analysis: Effects
of Adding Salmeterol to Inhaled Corticosteroids on Serious Asthma-Related Events. Ann Intern
Cates CJ, Cates MJ. Regular treatment with salmeterol for chronic asthma: serious
adverse events (Cochrane Review). Cochrane Database of Systematic Reviews2008(3).
Castle W, Fuller R, Hall J, Palmer J. Serevent nationwide surveillance study: comparison
of salmeterol with salbutamol in asthmatic patients who require regular bronchodilator
treatment. BMJ (Clinical research ed1993;306(6884):1034-7. 5.
Nelson HS, Weiss ST, Bleecker ER, Yancey SW, Dorinsky PM, the SMART Study Group.
The Salmeterol Multicenter Asthma Research Trial: A Comparison of Usual Pharmacotherapy for Asthma or Usual Pharmacotherapy Plus Salmeterol. Chest2006 January 1, 2006;129(1):15-
Weiss KB. Drug safety and salmeterol: the controversy continues. Ann Intern Med2008
Bateman E, Nelson H, Bousquet J, Kral K, Sutton L, Ortega H, et al. Meta-analysis: Effects
of Adding Salmeterol to Inhaled Corticosteroids on Serious Asthma-Related Events. Ann Intern
Cates CJ, Cates MJ. Regular treatment with salmeterol for chronic asthma: serious
adverse events (Cochrane Review). Cochrane Database of Systematic Reviews2008(3).
Castle W, Fuller R, Hall J, Palmer J. Serevent nationwide surveillance study: comparison
of salmeterol with salbutamol in asthmatic patients who require regular bronchodilator
treatment. BMJ (Clinical research ed1993;306(6884):1034-7. 5.
Nelson HS, Weiss ST, Bleecker ER, Yancey SW, Dorinsky PM, the SMART Study Group.
The Salmeterol Multicenter Asthma Research Trial: A Comparison of Usual Pharmacotherapy for Asthma or Usual Pharmacotherapy Plus Salmeterol. Chest2006 January 1, 2006;129(1):15-