Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
024 aetiology and patogenesis of acute high(75-86).pmd
AETIOLOGY AND PATHOGENESIS OF ACUTE HIGH ALTITUDE SICKNESS
Aetiology and Pathogenesis of Acute High Altitude Sickness
Analysis from the new scientific perspective of the Lung as a
mechanically active autonomic organ, under Vagus Sympathetic
Abstract Low air mass per volume unit at high altitude is the cause of acute mountain sickness.
The autonomic cyclic mechanics of the Lung start by contraction of the muscles of the
lobar bronchi and those of the lobular bronchioles, which while decreasing their capacities,proportionally increase the molecular mass per volume unit of the inspired air, thus increas-ing their molecular expansive forces.
These dynamics lead to displacement of the contained air in the sense towards lower
resistance, to then expand the pulmonary structures in balanced forces, once muscular relax-ation begins. Finally, the tiny intra-alveolar air masses distend the alveolar wall in balancewith capillary blood pressure.
These processes are accomplished by two kinds of dynamic cycles
Lobar cycles, for air renovation, under Vagus Nerve command.
Lobular cycles, for gas exchange with the blood, under Sympathetic Nerve
If the atmospheric mass of air per volume unit were lower to that demanded by the adap-
tation limits of the human specie, its molecular expansive force would be insufficient toachieve pulmonary dynamic expansion, with all that implies, as described above.
Therefore, the expansive molecular forces of the alveolar air mass would be insufficient
to expand the alveoli with the required tension to enable the right balance of blood and airpressure for balance for selective diffusion of Oxygen. The consequence would be pulmo-nary arterial blood hypertension, hypoxemia and pulmonary oedema, as is the case in AcuteMountain Sickness.
Simultaneous data and graphs of Resultants of these dynamics, discovered by the Author
in 1978, in the pleural space of experimental dogs, are analyzed. Related Author’s publishedworks are: “Fisiodinámica del Hombre en el Mundo” “The New Theory of RespiratoryDynamics” “Integración Dinámico Funcional del Organismo Viviente”. The Aetiology andPathogenesis of Acute Mountain Sickness
THE LUNG AUTONOMIC MECHANICS. THE HUMAN LIVING-BEING
We can identify, by abstraction, the origin of
some partial forces and their objectives.
This work, carried out during the year 2000,
obeys to my aim of applying the scientific basis of
1. Atmospheric force’s origin, relative
the Pulmonary autonomic mechanics, developed by
to altitude
me during more than twenty two years, tounderstand the Acute Mechanical failure of the
Altitude means distance from sea level, in es-
Lung dynamics at High Altitude, known as Acute
sence, distance from the centre of the Earth, from
which its gravitational force is exerted. This force,
contributing with its prevention and effective
applied on the Atmosphere, determines its length,
speedy treatment avoiding complications.
relative to the weight of its column of air, the valueof which at sea level is 76 cm Hg. Introductory Remarks
In other words: the mass of a column of atmo-
spheric air at sea level is 76 cm Hg and, from it,
Rigorous interpretation of this Discovery, which
approximately 21% corresponds to Oxygen, with a
represents a historical landmark, led me to define
partial pressure of about 15,96 cm Hg. And 79%
two different kinds of cyclic activity: One that com-
corresponds to Nitrogen, with a partial pressure of
prises the whole cycle, coincident with the breath-
ing cycles and the other, a series of minor cyclescoincident with cardiac cycles, both clinically de-
Now, this pressure corresponds to the lower levelof human adaptation in our natural habitat. If thepressure is increased for any cause, it will be in-
This complex Resultant is generated by cyclic
creased the Resultant force needed for the diffu-
variation of forces transmitted to the pulmonary
sion of gases, firstly Oxygen, surpassing the capac-
surface, which origin and development merit to be
ity of fixation by the haemoglobin of the blood and
Hence, applying the Newton’s Inertial Prin-
If distension of the alveolar structure increases
c i p l e F = m • a (force equals mass per
farther on, Nitrogen would also diffuse, with the
acceleration) it is compulsory to determine the
source of the forces, the identity of the mass, and
The mass of atmospheric air and with its pro-
the space limiting its acceleration, as well as the
portional masses of Oxygen and Nitrogen decrease
causes of the periods of those cyclic displacements.
during ascent from sea level, because the air col-
umn at each upper level diminishes. One most add
The Force
to this, temperature and humidity, among other fac-tors, with the consequences above mentioned.
The main working forces concurrent to the
These elemental concepts need no discussion.
performance of the Respiratory Cycles have twocomplementary sources, leading to complementary
2. Organic forces Origin Sources of the forces
1. Contraction-relaxation of the airways smooth
2. Expansive molecular force of the gasses
pressurised in each sector of the bronchial and
AETIOLOGY AND PATHOGENESIS OF ACUTE HIGH ALTITUDE SICKNESS
3. Capillary blood heat transfer to the alveolar air
sphincters, whose contraction generates the necessary
energy to decrease the diameters and length of thosepassages, with three main consequent effects.Diaphragmatic Belt of striated muscles.
1. Proportional reduction in their capacities.
5. Contraction-relaxation of the right ventricle.
2. Simultaneous proportional widening of the
structures are well known, as also are their muscular
3. Momentarily closure of the airways, by seg-
fibres distribution as geodesic networks andPhysiological objectives of the lobar bronchi muscular contraction
1. To increase pressure in the lobar bronchi
working effects of the Diaphragmatic Belt. That is
contained air, in accordance with the Boyle
to say, to evoke Diaphragm contraction, followed
Mariotte Principle V.P = C (Volume per Pressure
is a Constant.). This pressure increase means
(Diaphragm-intercostals and abdominal muscles2. accumulation of potential energy, as expansivemolecular forces.
3. To increase the pleural lumen, in order to
decrease resistance to pulmonary gases expansion
2. To generate Pulmo-diaphragmatic (Vago-Phrenic) mechanical reflex to incorporate the
Physiological objectives of the lobar bronchi muscular relaxation
1. Displacement of the previously pressurisedgases towards their destination on the pulmonary
3. Abdominal muscles contraction (Diaphrag-
periphery, by own molecular expansion, expandingmatic Belt), with press effect towards the thorax.the Lung, to accomplish immediate and mediateends.
4. Intercostals muscles contraction for thoraxDecrease resistance for Intra pulmonary gasexpansion (Diaphragmatic Belt), with flood- gateeffect, decreasing resistance to abdom- inal blood
2. abdominal press effect towards the lowThe mass.
The intrapulmonary working factor mass is the
the Trachea, where the air formerly inspired is pre-
mass of air contained in each sector of the air
acclimatised, that is to say, the mass per volumepassages, bronchial and bronchiolar, directly
unit of the atmospheric air is pre-adapted, along
renovated from the right and left main bronchi and
the extra pulmonary airways, to physical conditions
THE LUNG AUTONOMIC MECHANICS. THE HUMAN LIVING-BEING
Acceleration = e/t (space divided by time)
genetically programmed for use and final adaptation
The space is anatomically defined by the length
in the intra-pulmonary airways, while also
of one file of bronchi and bronchioles up to their
alveoli, while the time is physiologically determined
integrated physiological dynamic effects, for a final
by the period of the concerned cycles, which change
pulmonary result at the alveolar level, enabling
in relation with organic demands, under control of
Physiological Objectives of the Lobular Bronchiole’s Muscles contraction
Dynamics of the lobular bronchioles is similar,
ences relative to the magnitude of factors as well
in general sense, to the lobar bronchi, with refer-
Introduction
To understand the Aetiology and pathogenesis
of Species and Individuals Adaptation, which is
of AHAS it is necessary to know the normal dy-
genetically determined and infers the concept of
namics of the Lung in the habitat of natural adapta-
Altitude above sea level, this relative to the distance
tion of the species, as synthesised in the introduc-
from the centre of the Earth, as determinant of its
Gravitation Force and, with it, atmosphericpressure at different geographical levels, which is
Living species and individuals are mechanical
relative to the mass of air per volume unit.
structures genetically designed for dynamical inte-gration with the Atmosphere, at the very moment
Aetiology
of birth, and adaptation to different levels of alti-tude, within their own limits, relative to the mass
We are now starting focussing the Aetiology of
Acute High Altitude Sickness, which is relative tothe functional binomial Man-Earth of which the
It is well known that the respiratory function of
factor Man is the same and, only one element of
healthy individuals, in their local habitat, disposes
the factor Earth has changed: the distance from sea
of a wide adaptation range to organic demands,
level and its consequent effect on the mass per
volume unit of atmospheric air, which I pointed out
A wider concept of Habitat is Natural Habitat
Low air mass per volume unit above the upper limit of human natural adaptation is the
cause of the acute failure of the Lung dynamics known as Acute High Altitude Sickness
AETIOLOGY AND PATHOGENESIS OF ACUTE HIGH ALTITUDE SICKNESS
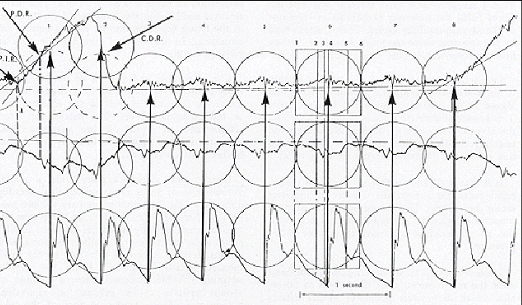
Fig 1. Simultaneous graphs of three main parameters from top to bottoms: 1. Respiratory Pulse: 2. Intra-pleural sub-atmospheric pressure abdominal aortic pulses. The circles defines each lobular alveolar-capillary cycle and thecorrespondences with the others parameters. The arrows mark the coincident inflexion of capillary and arterialpulses (Graph taken from my book “The New Theory of Respiratory Dynamics”2
Pathogenesis Mechanical Actions and Effects
Acute High Altitude Sickness is -+well known
1. Lobular Floodgate actions and effects in the
as the sum of signs and symptoms observed in oth-
erwise normal individuals when displaced at high
Retraction of the lobular structure, as a
altitude. Therefore, one needs to know how does
the binomial Man-mass of air at sea level works,
contraction, widens the pleural lumen to decrease
resistance to pulmonary arteriolar blood circulation
The Physical factor Man is represented in this
towards the alveolar capillaries. Floodgate action
moment of my analysis by the joint of the lobularunits of each and all the lobes in their ensemble, sincethe lobules receive the masses of air previously adapted
2. Lobular Press action by molecular expansion
along the airways and are the dynamic-functional units
of the air mass displaced up to the alveoli, distend
for development of the specific cycle leading to gas
the alveolar-capillary membrane, leading to:
exchange with the blood, while the alveoli are surfaceunits for Oxygen diffusion, under effect of theexpansive molecular forces of the tiny masses of gases
2.2 Press effect to displace the oxygenated blood
THE LUNG AUTONOMIC MECHANICS. THE HUMAN LIVING-BEING
the alveolar membrane, distorting Oxygen diffusion
distension generates two well-known signscharacterising the beginning of this sickness.
2. Pulmonary arterial hypertension, because low
alveolar-capillary press action, causing partial
1. Hypoxemia because insufficient distension of
retention of pulmonary arteriolar circulation.
Analytical Review of some clinical Data and Research
On the basis of the above general explanation, I
2.1 Oxygen diffusion, causing hypoxia and dis-
consider it useful to discuss now important clinical
placement of the Oxygenated blood causing retro-
and anatomopa- thologic observations carried out
grade retention of the pulmonary arterial blood, with
by different authors under various conditions and/
or stages of this sickness, but whose interpret-
The observation that acute administration of
ations, based on the traditional theory that consid-
Oxygen caused little or no fall in pulmonary vas-
ers the Lung a passive organ, has been unable to
cular resistance at rest and that Oxygen partially
define neither the cause nor the pathogenesis not
prevents the rise in pulmonary arterial pressure in
even the precise rational prevention and treatment,
exercise6 are also consistent with our mechanical
all of which constitutes the purpose of this work.
interpretation since the problem is not lack of Oxy-
Hurtado first demonstrated that pulmonary ar-
gen or hypoxia but lack of enough total air mass. If
terial hypertension in humans; this is a sign in pa-
acute administration of Oxygen prevents rise in
pulmonary arterial pressure is because the patientwas partially-adapted to that altitude and the addi-
Hurtado et all observe that Oxygen partially pre-
tional Oxygen supply the extra-demand because ex-
vents the rise in pulmonary arterial pressure in exer-
ercise, as in any patient suffering from respiratory
Arias Stella et all7, found that excessive muscu-
The excessive muscularity of the named arterial
larity of distal muscular arteries and arterioles is a
vessels is an expected anatomic-pathological con-
prominent feature of the pulmonary arterial bed of
sequence, because excessive repeated muscular
contraction to overcome the functional obstructiondue to lack of alveolar capillary press action and
Pulmonary hypertension and hypoxia are the
two most characteristic signs of the Acute High
Altitude Sickness because they are the two imme-
Peñaloza, Arias Stella et all8, observe that pul-
diate consequences of the mechanical unbalance
monary arterial pressure during childhood is higher
generated at the alveolar-capillary level, by means
of the two mechanical effects described above:
This observation obeys to the same mechanical
1. Increased Floodgate action by which aug-
ments the pulmonary artery blood towards the al-
Grover et all9 and Sime et all1 state that “pro-
longed removal of the hypoxic stimulus by descent
2. Decreased Press action because low expan-
to sea level result in the fall of pulmonary arterial
sive molecular force exerted by the alveolar air
pressure and pulmonary vascular resistance to nor-
mass, which prevents its two consequences:
AETIOLOGY AND PATHOGENESIS OF ACUTE HIGH ALTITUDE SICKNESS
The observations are correct, but the interpreta-
This pathology is generally interpreted as caused
tion is wrong. The correct interpretation must be:
by hypoxia, which is consequent with the prevail-
descent to sea level result in the fall of pulmonary
ing traditional theory of Respiration that considers
arterial hypertension and pulmonary resistance to
the lung a mechanically passive organ and, Oxy-
the arterial flow because the lung dynamics has re-
gen, as the gas useful for respiration, since this is
cuperated after restitution of a mass of air per vol-
the gas necessary for organic metabolism.
ume unit between the limits of natural adaptation.
Reaves and Grover11 observe that in newborns
Discussion.
breathing ambient air, the fall in pulmonary arte-
The Living being, is a complex integrated struc-
rial pressure during the first three days of life is
tural and functional organization, for maintenance
less marked than at sea level and Peñalosa et all12.
of created life in its natural habitat of adaptation,
Arias-Stella et all13 observe that throughout child-
hood pulmonary arterial pressure is higher at alti-tude than at sea level.
To achieve this purpose disposes of necessary
parameters for balance of actions, reactions and
Important observations. Their interpretations are
functional integrations, in the dynamic balance
characterising Life and Health, made objective as
Kronenberg et all14, observe that arterial pres-
sure in individuals coming from low lands in-
Let us now to analyse the posed problem, from
creased after a few minutes of exposure to altitudes,
the new scientific perspective of the Lung as a me-
reaching a plateau after 12 to 24 hours, being re-
chanically autonomic active organ working under
Vagus Sympathetic complementary command.
This observations are of theoretical and practi-
I discovered the autonomic. Resultant of cyclic
cal importance since they refers to a relative pe-
pressure variations of the pulmonary mechanics,
riod in which the strength for adaptation is near its
in its pleural surface (Respiratory Pulse) then, I
limit and Oxygen administration supply a little
analysed and interpreted its two main cyclic com-
Hurtado and others15-16 found that systolic pe-
One that embraces the whole cycle knew as
ripheral blood pressure was lower in practically all
"Respiratory", which is only relative to air renova-
tion from the Atmosphere, being generated by lo-
This very important observation is compatible
bar bronchial mechanics under Vagus control.
with re-distribution of the blood because of failure
The other, riding on the first: the lobular-alveo-
of mechanical factors developed by the thoracic-
lar-capillary pulses or respiratory pulses strictus
abdominal muscular and costal belt, as described
sense (pulses for gas exchange with the blood),
which are synchronous with the cardiac pulses2.
In synthesis, all these observations, as discussed
Forces for air impulsion and auto-impulsion into
here, are coherent with expectations derived from
the alveoli must balance the alveolar-capillary blood
my discoveries and their interpretations of pulmo-
pressure. The Sympathetic System coordinates this
nary mechanics, pulmo-cardiac dynamic integra-
tion, as well as with the integration and balance ofour organisms with the Atmosphere of the Earth.
I have fully described elsewhere the functional
THE LUNG AUTONOMIC MECHANICS. THE HUMAN LIVING-BEING
alveolar-capillary units, which represent the pulmo-Matter of discussion cardiac functional integration as a necessary con-dition. Consequently, obeying Sympathetic Adren-
The Living being, as a complex integrated struc-
ergic control, on a vagal dynamic basis. tural and functional organization, for maintenanceof created life in its natural habitat of adaptation,disposes of necessary parameters for balance of
Let us now to discuss the following:
actions, reactions and functional integrations, in thedynamic balance characterising Life and Health,
What does the concept Altitude mean, from the
scientific physic-mathematical analysis and, howdoes this affect the physiology of living beings,
We can pose the following questions.
1. How does Oxygen arrive or it is carried up to
Altitude means distance from sea level, in es-
the alveoli and, in which physical conditions, all of
sence, distance from the centre of the Earth, from
which subject to possible mathematical interpreta-
which its gravitational force is exerted. This force,
applied on the Atmosphere, determines its length,
2. What is the reason for those physical and
relative to the weight of its column of air, the value
In the light of my discoveries, analysis and in-
In other words: the mass of a column of atmo-
terpretations, the prevailing theory of respiratory
spheric air at sea level is 76 cm Hg and, from it,
mechanics does not give and can not give a single
approximately 21% corresponds to Oxygen, with a
rigorous answer since cyclic transportation of air
partial pressure of about 15,96 cm Hg. And 79%
masses obey pulmonary dynamic phenomena on one
corresponds to Nitrogen, with a partial pressure of
side and physiological demands on the other.
I have fully demonstrated, for over twenty-two
Now, this pressure corresponds to the lower level
years, not only that the Lung is an autonomous me-of adaptation in our natural habitat. If the pressure
chanically active organ, but also I have interpreted
increases for any cause, it will increase the Result-
this activity on a Physic mathematical basis, for
ant force needed for the diffusion of gases, firstly
Oxygen, surpassing the capacity of fixation by thehaemoglobin of the blood and the dissolved Oxy-
Atmospheric Air Transportation throughout the
Any Volume of inspired air, at any altitude has a
If distension of the alveolar structure increases
correlative mass. Volume-mass that must be dis-
farther on, Nitrogen would also diffuse, with the
placed throughout the airways in conditions of pres- sure, humidity and temperaturephysiologically
On the contrary, the mass of total air and the
determined, du- ring a time relative to the integrated
proportional masses of Oxygen and Nitrogen de-
simultaneous rhythms, generated by their autono-
crease during ascent from sea level, since the air
mous innervations, which also determine the con-
column diminishes. One most add to this, tempera-
tracting force of the airways muscular fibres, gen-
ture and humidity, among other factors, with the
erating proportional variations in their respective
consequences above mentioned. These elemental
capacities and also simultaneous closure, due to
sphincters action (sphincterlike of Miller).
AETIOLOGY AND PATHOGENESIS OF ACUTE HIGH ALTITUDE SICKNESS
This mechanics is the essence for air transporta-
bres disposed as sphincters, on contracting in re-
tion, since according to Newton's Inertial Law, I
sponse to Vagal and Sympathetic nerves discharges,
repeat, any displaced mass is a result of a force ap-
decrease the capacities of their corresponding air-
plied on it, which exerts an acceleration ex-
ways, also closing them momentarily. Conse-
pressed by the equation F = m • a, from which
quently, this muscular contraction proportionally
the equations m = F/a and a = F/m. Are de-
pressurise the contained air masses, increasing their
mass per volume unit (Boyle-Mariotte Law) alsoaccumulating expansive potential forces to be used
The space for displacement of the air mass does
not change, since this is the length of the namedairways.
When muscular relaxation starts, the expansive
force of the gas molecules of the air, previously
pressurised, displace themselves in the sense oflower resistance, that is to say towards the destina-
1. Volume-mass of air, relative to pulmonary ca-
tions programmed in the organic design, immedi-
pacity and altitude above sea level.
ate and mediate, the alveoli being their final pul-
2. Forces generated by cyclic muscular contrac-
tion on the pulmonary structures, to vary their own
The mass of inspired air is simultaneously dis-
capacities and, therefore, their contained air mass
placed throughout the different sectors, bronchi,
per volume unit, accumulating potential forces to
bronchioles, during simultaneous and successive
be used during the following phase of muscular re-
I have defined four periodical sectors: 4.
3. Rhythms of nerve discharges for integration
Coordination of these dynamic factors are nec-
essary for simultaneous displacement of the vari-able masses per volume unit, towards intermediate
and final destinations, in required physical (physi-
I shall avoid here the two first sectors, explained
ological) conditions; to enable selective diffusion
apart, and will only refer to the third and fourth,
of Oxygen in the required amount, to satisfy the
which are closely related to specific pulmonary
demand of load by the haemoglobin of the red cells
structures and constitute the first dynamic step of
simultaneously circulating throughout the alveolar
Inspiration: air renovation throughout the air-
The previous paragraphs contain the utmost fac-
tors of the problem and pose the need for an expla-nation about the how's and why's of the variables
Relaxation of the lobar bronchial muscles gener-
and their conditions, with physic mathematical per-
ate a sucking force against the air masses supplied bythe right and left major bronchi. Those masses of airshall fill the capacities left empty by the former dis-
The smooth muscular networks of the airways,
place- ment of the air masses retained for
correlative to the local and integrated functional
acclimatisation during the former cycle. This process
tasks of bronchi and bronchioles, included the fi-
is simultaneously followed by displacing the air now
THE LUNG AUTONOMIC MECHANICS. THE HUMAN LIVING-BEING
filling the upper airways and finally the air from the
Simultaneously, the lobular structure retracts to
Atmosphere. This latter is the only objective act de-
open ways for arteriolar blood circulation towards
fining Inspiration in the traditional sense5.
the capillaries. The molecules of gases shall expand,distending the alveolar capillaries membrane in
The next muscular contraction, due to the Va-
balance with blood pressure, thus enabling selec-
gus nerve discharge will decrease the bronchial ca-
tive diffusion of Oxygen in the amount programmed
pacity thus pressurising the intra-bronchial mass of
in the structural design, under Central Nervous
air. This fact is followed by muscles relaxation,
System control. This expansion also works as a
opening ways for the air mass displacement towards
press to displace the oxygenated blood towards the
the pulmonary periphery, in order to supply the
quote of air demanded by each and all the lobules.
It is obvious that if the mass per volume unit of
Simultaneously, the same muscular contraction,
the inspired air is inferior to that required by the
when retracts pulls from the parietal pleuras, wid-
dynamics in progress, the effects produced by the
ening the pleural lumen, creating potential space
actions and reactions derived from the muscular
for pulmonary gases expansion with to effects flood
increased contrac- ting force, will become propor-
gate and press action to balance fluids circulation.
tionally increased and, even with the maximal ef-
The lobular units repeat the lobar process, but
fort of compensation facing the final balance, Oxy-
under Sympathetic nerve discharges, with their own
gen diffusion will not suffice, and the anoxic effect
intensity and rhythm, thus, widens the pleural lu-
will occur. Besides, parallel mechanical effects gen-
men to open ways to arteriolar blood circulation-
erating signs and symptoms characterising Moun-
floodgate action- and simultaneous pulmonary ex-
tain Sickness will also be produced, these latter
pansion. The lobular bronchiole's muscular relax-
mechanical effects generally ignored until now.
ation sucks small masses of air supplied by the nextlobar bronchi, then pressurises them by muscularcontraction. This process leads to circulation to-
It is clear that the anoxia in the tissues is a con-
wards the capillaries and the air displacement to-
sequence of the primary mechanical problem gen-erated by insufficient mass of inspired air.
I must emphasise the fact that the posed general problem is Insufficient air "mass",
in relation to that required by the pulmonary functional structure, which is designed
to generate and develop the mechanical process needed to achieve the functions
enabling Life and Health in the natural environment of adaptation of the species and
The air mass per volume unit supplied at higher altitudes to that of the species adapta-
tion limits results insufficient to distend the pulmonary structures and further along, the
alveolar-capillary membranes, generating organic dynamic unbalance.
AETIOLOGY AND PATHOGENESIS OF ACUTE HIGH ALTITUDE SICKNESS
The functional insufficiency becomes evident
mass of air per volume unit, at the human adap-
once the potential capacity of action of the pulmo-
tation limit is the physic-natural factor for inte-
nary structure is exhausted. It is necessary to insist
gration and balance, when satisfying the organic
that the maximal nervous discharges enhance maxi-
demand for its basic physiological performance,
mal muscular con- tractions, able to decrease the
accomplishing the equation of the Inertial
bronchial capacity up to the limit allowed by the
structure of cartilages, which guarantee the perma-nent filling by "residual air" as a condition for ho-
Life in health is the natural consequence of in-
tegration and balance of two primary factors:
Let's now think in another simultaneously im-
portant problem. The pulmonary blood vessels are
2. The Atmosphere of the Earth, between the geo-
distributed in parallel with the airways and, elastic
graphic limits of adaptation of the specie, which
and collagen fibres surround both kinds of passages,
supplies the air mass per volume unit that corre-
making them co-participant in common mechani-
sponds to the organic genetic design. Acute High
Altitude Sickness is the joint of signs and symp-toms derived from organic dynamic insufficiency
Prevention.
due to a mass of air supply inferior to that requiredfor the organic dynamic balance.
It is necessary to know the maximal altitude of
physiological adaptation of the Human Living
The Living Being is a functional structure de-
Being's vital structures and, to make aware that if
signed to maintain the created life in its natural
that limit is surpassed, individuals must be provided
with chambers or tents of total pressurised air, rela-tive to the adaptation level of the group or indi-
The natural habitat of the humans is the surface
of the Earth and its Atmosphere, between limits ge-netically established.
Administration of pure Oxygen has been widely
used in prevention and even in therapy, as result of
The Lung is the organ responsible for this dy-
the fact that the autonomic pulmonary mechanics
namic integration.
and its direct relationship with the gaseous massof air are still unknown. As a consequence, the re-
The pulmonary lobules are the structures to ac-
sults have not often been satisfactory and, when
complish the final step of the necessary balance, at
they look like being, it would be interesting to
analyse the conditions of the individuals as well as
The two factors integrate dynamically at the very
all the conditions implicit in the supplied measures.
moment of berth, direct and primarily by the pulmo-nary functional structure, in its thoracic ensemble. The
Conclusions
factor of integration and balance of the pulmonary dy-
Living Beings in the environment of their
namics and Universal dynamics is the air mass per
natural integration and adaptation, constitute an
volume unit, which is relative to the altitude also rela-
Organic-Physical Natural-Unit genetically de-
signed to accomplish basic dynamic functions
The tiny masses of air distributed among the al-
as an Autonomic Balanced Mechanical System
veoli exert expansive forces to distend the alveo-
of Fluids, for which the inspired atmospheric
lar-capillary membranes, with two objectives.
THE LUNG AUTONOMIC MECHANICS. THE HUMAN LIVING-BEING
1. To widen the pores of diffusion to open way to
crease in the bronchiolar muscles contraction up to
the Oxygen molecule and not to that of Nitrogen.
the potential limit, after which hypoxemia and pul-monary hypertension with alveolar infiltration and
2. To simultaneously perform press action to dis-
place the oxygenated blood towards the pulmonaryveins.
If the problem persists, the organic dynamics far-
ther than the pulmonary limits, starts to manifest
Scarce air mass determines compensatory in-
References
1. González-Bogen A. "Fisiodinámica del Hombre en el
9. Reynafarje, C. Sánchez and J. Muñoz. Report to the USAF
Mundo" 1979. Ediciones de la Biblioteca UCV. P.O.Box
10. Grover, R.F., Hill, D.H., Reeves, J. T., Weir, E.K.,
2. González-Bogen A. "The New Theory of Respiratory Dy-
McMurtry, I.F., & Alexander, A.F. (1975) Pulmonary hy-
namics". 1985. Ediciones de la Biblioteca. UCV.
pertension at altitude. Progress in respiratory research,vol. 9 pp 112-117. Karger, Basel
3. González-Bogen A. "Integración Dinámico funcional del
11. Sime, F., Peñaloza, D. & Ruiz, L.(1971) Bradicardia, in-
Organismo-Viviente" 1989. Ediciones de la Biblioteca.
creased cardiac output, and reversal of pulmonary hy-
pertension in altitude natives living at sea level. British
4. González-Bogen A. International Seminar "The Respi-
ratory Pulse" Scientific Review. 1992. Year 1. Nº1. 1992.
12. Reeves, John T., Bertron M. Groves, John R. Sutton, Pe-
ter D. Wagner, Allen Cymerman, Mark K. Malconian,
5. González-Bogen A. Web site http://www.the-respiratory-
Paul B. Rock, Patricia M. Young, and Charles S.
13. Peñaloza, D., Sime, F., Banchero, N., Gamboa, R., Cruz,J.,
6. Rotta, A., Cánepa, A., Hurtado, A.,Velazquez, T., &
and Marticorena, E.: Pulmonary hypertension in healthy
Chavez, T. (1956) Pulmonary circulation at sea level and
men born and living at high altitudes. Am. J. Cardiol.
at high altitudes. Journal of Applied Physiology, 9, 328-
14. Arias-Stella, J., and Kruger, H., Pathology of high alti-
tude pulmonary oedema. Arch. Path. 76: 147, 1963.
7. Arias-Stella, J. & Saldaña, M. (1963) The terminal por-
tion of the pulmonary vascular tree in people native to
high altitudes. Circulation, 28, 915-925.
16. Hurtado, A., Merino, C. and Delgado, E. Arch. Int. Med.
8. Peñaloza, D., Arias-Stella, F. Sime F., Recavarren, S. &
Marticorena E. (1964) The heart and pulmonary circula-
17. Hurtado, A., T. Velazquez, C. Reynafarje, R. Lozano, R.
tion in children atn high altitudes. Pediatrics, 34, 568-
Chavez, H.Aste Salazar, B. Reynafarje, C. Sánchez and
J. Muñoz. Report to the USAF School of Medicine, 1954.
Pain Management Partners LLC- James R. Morris, MD 2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631 Name: _____________________________________ Date: ____________ Birthdate: ________ Who referred you? ______________________________________________ Phone: __________ Who is your treating physician now? ________________________________ Phone: __________ Describe the pain you
ippg.com Physiology A Recollected questions of 8. BMR in a 40 kg man is PGI DECEMBER 2001 send corrections to contribute@aippg.com a. starvation decreases BMR by 50% b. starvation increases BMR c. independent of hormonal influence a. Common hepatic b. Right hepatic c. Left hepatic 11. Ca+2 metabolism organs do not take part c. sept from third ventricle by pars art c. left b
 AETIOLOGY AND PATHOGENESIS OF ACUTE HIGH ALTITUDE SICKNESS
Fig 1. Simultaneous graphs of three main parameters from top to bottoms: 1. Respiratory Pulse: 2. Intra-pleural sub-atmospheric pressure abdominal aortic pulses. The circles defines each lobular alveolar-capillary cycle and thecorrespondences with the others parameters. The arrows mark the coincident inflexion of capillary and arterialpulses (Graph taken from my book “The New Theory of Respiratory Dynamics”2
Pathogenesis
AETIOLOGY AND PATHOGENESIS OF ACUTE HIGH ALTITUDE SICKNESS
Fig 1. Simultaneous graphs of three main parameters from top to bottoms: 1. Respiratory Pulse: 2. Intra-pleural sub-atmospheric pressure abdominal aortic pulses. The circles defines each lobular alveolar-capillary cycle and thecorrespondences with the others parameters. The arrows mark the coincident inflexion of capillary and arterialpulses (Graph taken from my book “The New Theory of Respiratory Dynamics”2
Pathogenesis